When food becomes medicine
This article is part of our special series on Flesh
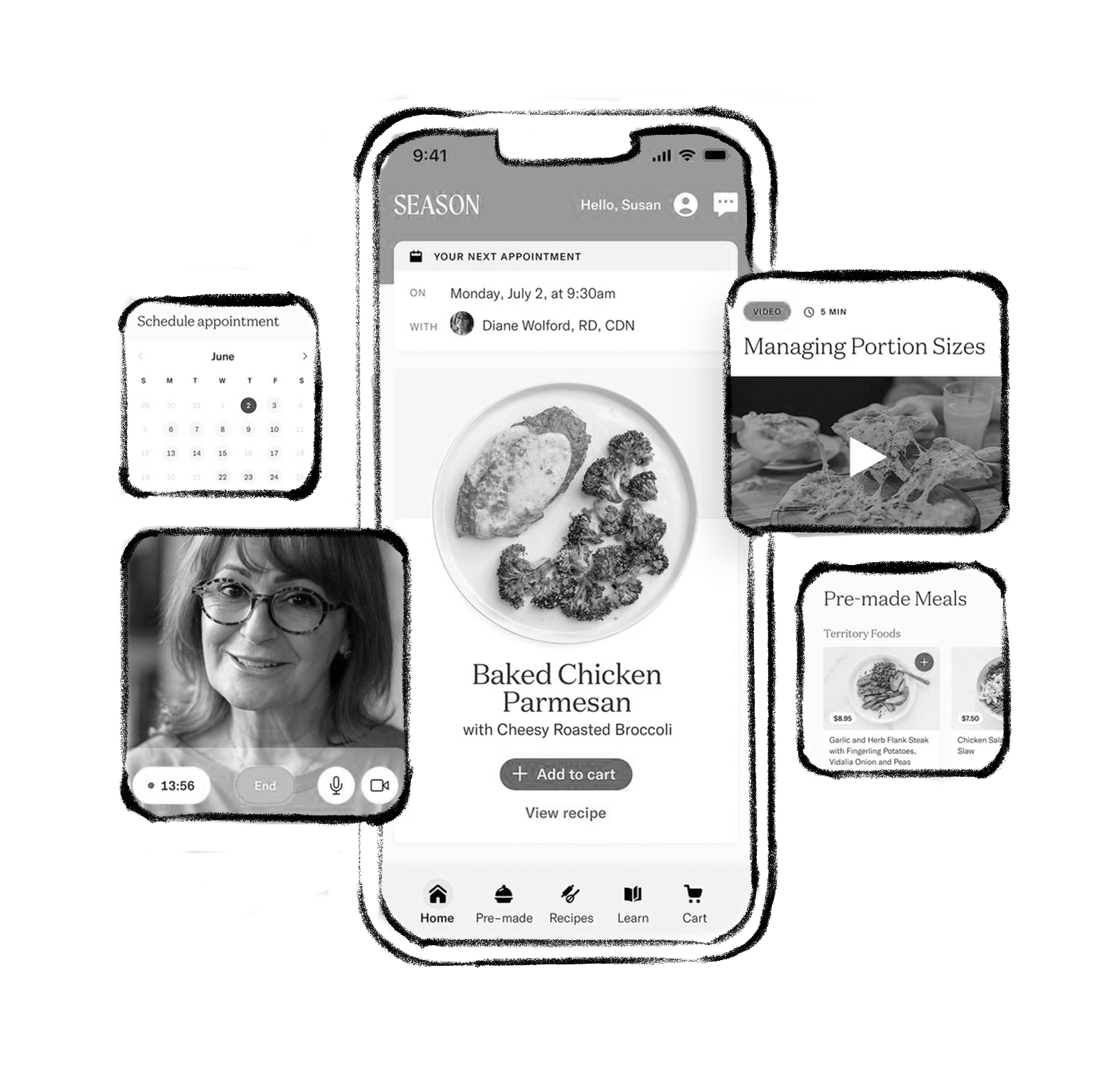
ReD partners Ian Dull and Anne Mette Worsøe Lottrup spoke with Season Health’s Josh Hix (CEO) and Morgan Flannery (SVP of Strategy) about the success of their food-as-medicine business. Season Health is the only integrated Food-as-Medicine Platform that drives engagement, health outcomes and total cost of care reduction for individuals, health plans and employers across populations. By combining evidence-based clinical care with access to affordable medically-tailored meals and groceries, Season Health empowers individuals and their families to make informed, sustainable choices, measurably improving both health outcomes and quality of life. In this interview, Josh and Morgan speak about how they started their food-as-medicine platform, adherence, and the challenge of introducing new approaches to healthcare.
Ian Dull: For many years across our work in healthcare, biotech and food, ReD has observed shifts towards more holistic definitions of well-being, nutrition, and more. Food has seen especially strong shifts in recent years, with consumers rapidly adopting more whole and fresh foods, building a vocabulary around ‘healthier’ processing, and exploring new ideas like the gut microbiome. Now, the idea of ‘food as medicine’ is gaining steam. How did Season Health get started?
Josh Hix: Originally I built a food company, just a pure food company. No functional benefits, nothing. We were a meal kit company. About halfway through building that, folks reported that they were healthier because they started using this product; for example, their diabetes was better controlled, so a very measurable thing. So we spent some time with them, interviewing patients and built a thesis. Many years later, after selling the food company and while I was figuring out what was next, that felt like a piece of unfinished business. Now, we serve health plans, they’re our customer, but who we really serve are their members living with chronic disease. Those are the people that need the most help. So I think the right way to build the business is to focus on the folks that need the help, which enables us to build the product, so that one day, years down the road, we can offer that product to people who are healthier. You start with the Roadster or the iPod or whatever in order to evolve to the next thing.
Anne Mette Worsøe Lottrup: One of the biggest questions I have relating to the work we do in healthcare is around adherence. People know that they’re sick, they know they need the medicine, their life is potentially dependent on taking it, but still adherence remains a big problem to solve. I wonder, what did you bring into your platform to fix that problem?
Josh: I think that the big difference is that you don't have to take medication, but you do have to eat. So there is adherence. But then the question is, can you shift those eating habits? It actually turns out that especially for the sickest folks, changing their diet even a little bit or what seems like a little bit – 3 to 5 meals a week, let’s say – has a huge impact. When we were interviewing folks in the Plated years, we often heard them say, “I eat fast food five times a week,” but then their household made a change. They still go to fast food two nights a week, but on the other three nights, they’re making food at home or ordering from Plated. And by the way, what they’re ordering from Plated is still burgers and pizza. But the difference between the fast food meal and the meal that they were making from Plated is that the Plated meal generally uses more whole foods: whole wheat buns on the burger, less sugar in the ketchup, smaller portions, etc. It’s almost sort of like a magic trick, like a sleight of hand, they don’t even know it’s happening. And yet, six months later they’ve lost weight and feel better. Nobody even notices they made a change. One of the big inputs into thinking about adherence is making it good – if the food’s good and it’s around you, you’ll eat it. If you have good food that the family likes, healthier versions of something that’s familiar, of course that person would get healthier. So we’re helping to change that household food environment and to some extent we’re achieving that goal. The food that is in the house is all of a sudden incrementally healthier in familiar ways. The outcomes at this point are amazing; we have 85% engagement through the end of our six month programs.
“One of the big inputs into thinking about adherence is making it good – if the food’s good and it’s around you, you’ll eat it.”
Ian: When does food become medicine in your mind?
Josh: I guess there’s no one definition or specific definition to that. But I think where I would start is with the dietitian. That’s where the real clinical healthcare intervention starts. They’re prescribing nutrition to the person. I think that’s the most “medical” part of the whole equation. There’s almost universal agreement about the food that is bad for us, but there is approximately zero consensus on what’s good for us. It’s not an exact science, which makes it really hard. For example, do blueberries actually help you live longer? I don’t really think anybody thinks they’re bad for you, but whether they’re actually good for you in any kind of longevity sense is a shockingly unanswered question. And so when we think about medicine, what we’re doing is saying “eat less food that is poison” more than “eat food that is medicine”, if that makes sense. So for us, the medicine is more in the subtraction of bad stuff.
Anne Mette: It sounds like your approach is: “How do I make incremental small changes around a person to make them more healthy,” such as having a dietitian that understands what kind of food they normally make, and then making a version of that and removing all those practical barriers for it to be done in real life.
Morgan Flannery: Exactly. The other thing that I think makes us quite different from a lot of the solutions out there across the spectrum is that we actually also invest a lot in measuring outcomes. So we’re sending home lab kits, blood pressure cuffs, digital scales. We’re evaluating CGM [continuous glucose monitor] integrations now. Most of the incumbents in the space don’t do that. And so it’s hard for them to say, “Oh, this is medicine” and not have any research around whether or not it’s working.
Josh: As Morgan said, we’re planting ourselves in the medical space by measuring outcomes, using only evidence-based diets and letting the clinician make the decision for and with the patient. But net variety is the real answer. We have nearly 300,000 recipes on the platform, and the point is to put the person on a diet that works for them. It has to be food they like, and that is going to drive the health outcome they need. A diversity of backgrounds for dietitians is therefore really important – both culturally and in terms of how they treat folks.
Ian: You must be in conversations with payers and insurers all the time at this point. Why are they interested now in exploring these kinds of health plans?
Josh: On one level, it’s nothing new. But I think that the current round of attention that food as medicine is getting is in many ways related to Covid-19. And it’s hopefully a silver lining. I think Covid-19 really drew attention to the down side of cardiometabolic and other chronic diseases. By some estimates, 90% of Americans are metabolically unhealthy. So it’s a staggeringly huge cost to everybody in both human and financial terms. Then on the food side, the consumer side, it’s kind of a similar story. Our grandmothers were probably not ordering Instacart before Covid-19. What the news cycle did for 18 months was tell people that going to the grocery store might literally kill them. And so everybody learned how to use Instacart and UberEats and DoorDash and QR codes and all of these things. All the food companies had to adopt them. We transitioned to a world where the most vulnerable were doing telehealth visits and ordering food online, and that created the necessary conditions to be able to build what we’re doing now. The White House had the first nutrition summit in 50 years last year, and this self-fulfilling swirl of energy is generating the focus on the space.
Ian: In terms of convincing payers to get on board, they’re always going to have some of these holdouts who may just be looking for evidence in their state or with a particular population. Has that been changing? Are people more open to experimenting with folks like you or others who bring in different types of behavioral change programs and new types of therapies?
Morgan: The short answer is yes. We’ve seen changes, particularly around food. One is macro, which is the governmental policies put in place since 2020 that just made covering food as a benefit more legally possible. For example, in 2020, CMS issued something called the SSBCI Benefit which basically allowed a plan to target a benefit for a particular cohort of their population, based on clinical need. So there’s a policy angle. I think the other thing that we spend a lot of time on is targeting some of the regional Blue Cross Blue Shield plans. Those plans tend to be more innovative in this type of space because they have much more dominant market share. In a way, they are “cradle-to-grave” plans, meaning they are likely to cover an individual through the course of a much longer time period. And so they’re willing to take a leap of faith in investing in solutions that might take longer to play out.
“When we think about medicine, what we’re doing is saying ‘eat less food that is poison’ more than ‘eat food that is medicine’.”
Ian: While many treatments are very much focused at the individual level, we see in a lot of our work across healthcare that it is often treatments rooted in a community, a family, friends that have the most longevity. And food is one way that brings people together. Are you consciously thinking about that in the offerings you have been building?
Josh: Very consciously. Of course you have to address the household. Asking anybody in the house – especially if it’s the person responsible for buying food – to do something different is a losing battle.
This podcast is part of our special series on Flesh